Overselling overpronation
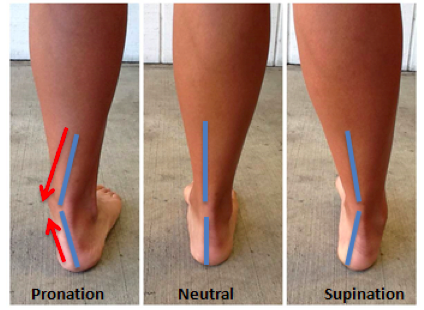
 Recently I was alerted by the internet “fact” that 90% of the general population’s feet are over-pronated. Pronation is the motion of the foot as it roles inward after the foot makes contact with the ground. Overpronation causes the arch of the foot to flatten excessively placing stress and pressure on tissues and ligaments of the foot. Over-pronation , flat foot, pes planus, fallen arches has been worried to lead to many foot problems including plantar fasciitis, ankle pain, lower back pain etc.
Recently I was alerted by the internet “fact” that 90% of the general population’s feet are over-pronated. Pronation is the motion of the foot as it roles inward after the foot makes contact with the ground. Overpronation causes the arch of the foot to flatten excessively placing stress and pressure on tissues and ligaments of the foot. Over-pronation , flat foot, pes planus, fallen arches has been worried to lead to many foot problems including plantar fasciitis, ankle pain, lower back pain etc.
Various websites mainly selling foot orthoses or related products claim 60% and even up to 90% of the population “suffered” from this condition, and should be corrected. However, a medical review on its prevalence found mostly on children, with quite a high variation estimates from less than 1% to as much as 78%. A Cochrane review concluded that “Flat foot is often unnecessarily treated, being ill-defined and of uncertain prognosis.”
Not all people with over-pronation have problems. A study published in 1993 evaluated foot morphology and injury risk in 246 male army recruits followed during 12 weeks of intensive training. They found that 20% of trainees with the flattest feet had the lowest injury risk. In contrast, the 20% with the highest arches had a 6-fold greater injury risk than the flat-footed group. The middle 60% of trainees had an intermediate risk. This study dispels the notion that flat-footed people are prone to injury during exercise. But people with high arches should be advised to pursue non – weight-bearing exercise, particularly if they have a rigid deformity.
Matt Wallden, an osteopath from the UK, in a publication published in Journal of Bodywork and Movement Therapies, suggested that there’s no such thing as a flat foot, only a lazy or deconditioned foot. He challenged the idea that the necessity on the use of foot support, as “to support a biological structure, in the long term, is to weaken it”.
Matt Wallden proposed using a credit or business card test, which was designed to screen for subtalar joint neutral by podiatrist Michel Joubert. The client in a normal standing posture, place a credit or business card alongside the lateral border of the foot in alignment the lateral malleolus. When the talus is palpated to be in subtalar neutral, this means that the lateral malleolus is in direct vertical alignment above the lateral border of the foot. The distance between the vertical border of the credit card and the lateral malleolus is a measure of the degree of static pronation, which usually ranges from between 5 to 15 mm. The credit card test is an easy and objective test for static subtalar pronation, the distance from lateral malleolus to vertical border of the credit card can be measured in millimetres.
To remedy this condition, Matt proposed the use of a foam roller longitudinal exercise, which “trains the nervous system not doing the job it should do; in combination with a likely concomitant deconditioning of the muscles”.
He described the exercise balancing on an unstable surface as follows:
The client lies down on a foam roller in a longitudinal position with knees flexed to support the body and feet flat against the floor. This condition may already create an instantaneous change in the foot posture because the foot needs to balance the body and bears less weight. The next challenge is to ask the client to place her hands across the chest and to lift one foot off the floor. This creates another level of balance challenge and simultaneously unloading the foot. As the foot on the ground needs to establish stability, it automatically attempts neutralize its subtalar position by “switching on” the intrinsic muscles of that foot, leading to the reformation of the arch. The credit card test can be re-evaluated after the exercise.
Note that there various causes of overpronation, and the above exercise is only for training “weak” muscles. When a client has an indication of overpronation that needs to be addressed, the cause needs to be tackled first before pursuing with treatments.
References
Burns J, Crosbie, J., Ouvrier R, Hunt A. Effective orthotic therapy for the painful cavus foot. Australasia J Podiatric Med, 2006; 40 (3): 61-6.
Cowan DN et al. Foot morphologic characteristics and risk of exercise-related injury. Arch Fam Med 1993 Jul 2 773-777.
Evans, A.M., and Keith R. A Cochrane review of the evidence for non-surgical interventions for flexible pediatric flat feet. Eur J Phys Rehabil Med 47 (2011): 69-89.
Matt Wallden. Don’t get caught flat footed – How over-pronation may just be a dysfunctional model. J Bodyw Mov Ther. 2015 Apr;19(2):357-61.