ITB: Our methods still get results; it’s our explanations that need updating —Til Luchau
Thanks for the opportunity to comment on the ITB studies and controversy. I’ve been watching this debate from a distance since the shrill social media posts about it began to appear a few years ago, and now that you’ve called me out, I enter the fray with a bit of caution, since I am a practitioner and trainer of practitioners, and not a researcher or academic per se. But here’s what stands out to me in reading over the studies, posts, and comments:
- It’s interesting (though not exactly revolutionary) that the Falvey study described the ITB as a thickening of the leg’s surrounding fascia latae, “rather than a discrete entity.” (Of course fascial anatomists have been saying this about all fascial structures for quite some time now, but great to see it in a non-manual therapy study).
- Similarly, it’s interesting that the ITB was found to attach to the femur along its entire length. This is different from the impression gained from conventional 2-dimensional anatomy illustrations, but is consistent with what can be seen in 3D imagery, such as the Visible Human Project’s data set (Figure 2, used in our trainings as well as in Tom Myers’ and others), and with cross-sectional images going back to Grey’s 1918 anatomy atlas (Figure 1). In cross-section, the ITB is barely visible, and is seen as the surfacing of a deep inter muscular septum, rather than a discreet band on the side of the leg.
Figure 1. Cross section of the human leg (from Gray’s Anatomy).
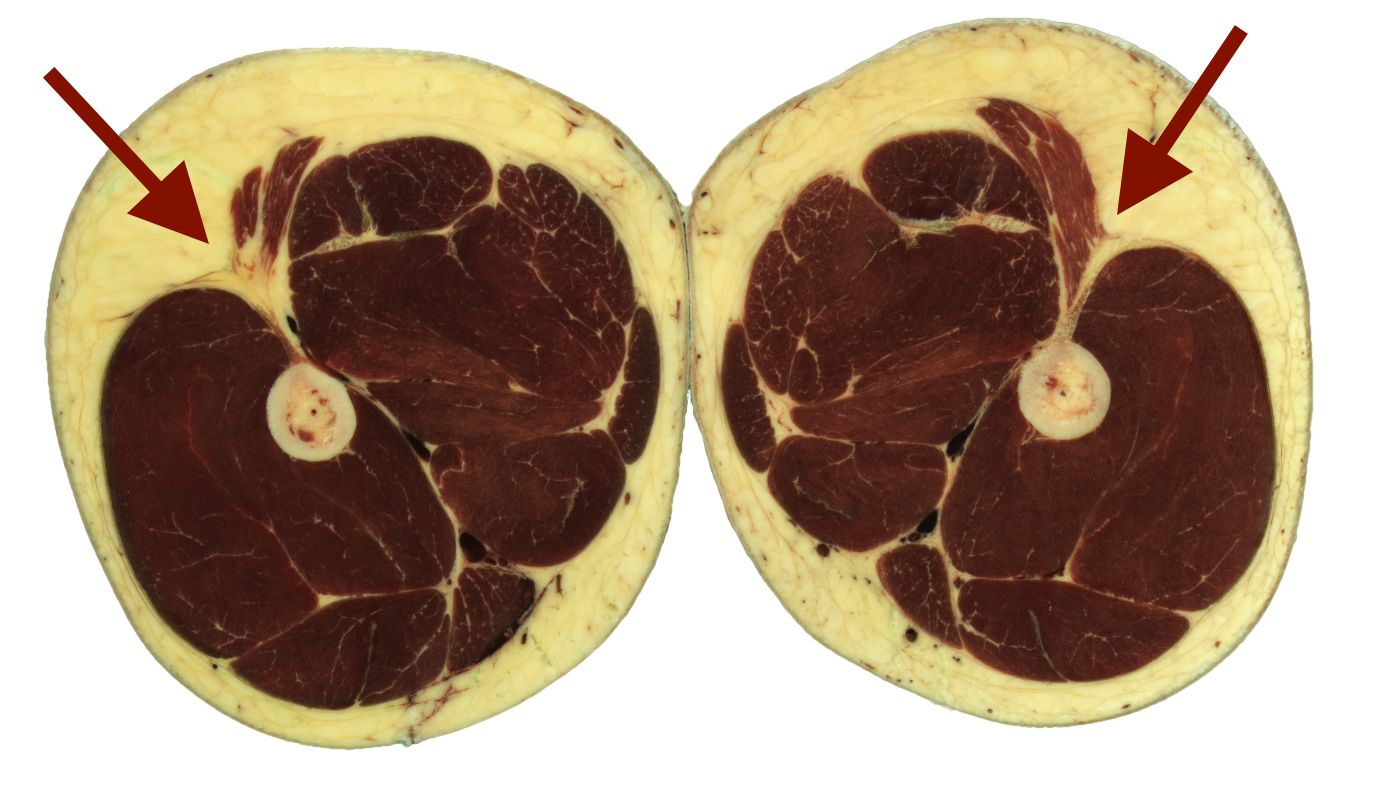
Figure 2. Cross-section of the human leg, mid thigh, arrows indicate the location of the ITB which extends deep within the leg via an intermuscular septum that attaches it to the femur along its entire length. Image from the Visible Human Project.
It’s fascinating that no ITB bursas were found in any of the cadaveric specimen. If this holds true for living bodies (and in those younger than the study’s average age of 76 years old), then it suggests that explaining lateral knee pain as bursal irritation needs re-thinking.
3. Like Joe Muscolino says in his comments, I’m not uncertain if results from tissue-stretching and strain experiments on elderly cadavers can be directly applied to living bodies of all ages. But it is not surprising that the ITB was found to be impossible to lengthen much by stretching. The ITB is a tendon, its thus its function is probably to transmit or to store tension, rather than modulate tension by lengthening as a muscle belly would. (Interestingly, here is a small study that suggests foam rolling decreases jump performance, at least in the short term: http://digitalcommons.sacredheart.edu/masterstheses/2/, though it does conclude that ITB rolling can be beneficial in injury recovery.)
4. It makes sense to me that rolling would not “stretch” the ITB (even if it was stretchable), or differentiate it from its surrounding tissues (which is one of the things we think we’re doing in our Advanced Myofascial Techniques approach). Greg Lehman (who’s iconoclastic perspectives I do enjoy, even though he probably throws a lot of babies out with his bathwater) says about this issue “I can’t fillet a chicken breast with a rolling pin.” In other words, mashing the ITB may or may not have some benefits, but stretching or separating it from its surroundings probably aren’t the explanations for why ITB rolling helps (or hurts).
5. This issue aside, in my reading over the abstract and the debates, I don’t find any logic that supports NOT rolling the ITB, unless you’re 1) overdoing it, or 2) doing it right before a performance event involving jumping. In fact, many authors sceptical of the stretching theory allow that there may be addition benefits not explained by stretching. So instead of one of the studies author’s blog post title, “Ilio-tibial Band: Please do not use a foam roller! , a more logical conclusion might be “Rolling (probably) does NOT stretch the ITB, but don’t over-do it!”
6. In my hands-on practice, I don’t feel much if any stretch when I work with the ITB, though I often think I feel a change in ITB tissue resilience, density, and differentiation. And of course, clients report a change in movement, lateral leg proprioception, and pain as a result of hands- on work, and often, from rolling their ITB’s themselves. There are several possible explanations for what I feel, and for the improvements my clients report, with influences on the nervous system being the primary suspects, and any actual change in the tissues’ physical properties being secondary.
After reading the different views on ITB work, I went and wrote more about my own views as an article for the May-June 2016 issue of the Massage & Bodywork magazine here. (See also the video here https://youtu.be/wYQTcRRugBE)
So in conclusion, here’s more evidence to suggest that our tissue-based models of manual therapy’s effects might be less accurate than we thought. But, that doesn’t mean that the old ways don’t get results; it just means we need to stay open-minded about our explanations about how they do their good. And once we get clearer about the new models, they’ll doubtless inspire new ways of working that we might not have imagined under the old models.
Til Luchau, Advanced-Trainings.com, is a Certified Advanced Rolfer and the originator of the Advanced Myofascial Techniques series.
Read also
- Iliotibial Band Syndrome: ITB cannot be stretched
- ITB: Empirical evidence is the reality—Robert Baker
- ITB: Extrapolating results from research to hands-on manual therapy should be done with caution—Joe Muscolino
- ITB: Our methods still get results; it’s our explanations that need updating —Til Luchau
- Can you stretch the ITB?
Effects of Acute Exercise on Remodeling of the Skeletal Muscle Extracellular Matrix Gene Expression