Isometrics for Tendon Pain – Practical implementation and considerations
Isometrics for Tendon Pain – Practical implementation and considerations
By Ebonie Rio, Craig Purdam, Sean Docking & Jill Cook
Tendinopathy, pain and dysfunction in the tendon, can be difficult to treat. Traditionally eccentric exercise has been used in the rehabilitation of tendinopathy and has been shown to be superior to concentric only and passive treatments. However, there are many instances where the use of eccentric exercise is unhelpful or in fact detrimental, for example the in-season athlete where adherence is poor or pain may increase. Even those who work with the non-athletic population know that adherence is a challenge as eccentrics are painful to complete 1.
Recent research has demonstrated a positive effect (reduced tendon pain, reduced motor inhibition and improved muscle performance) following isometric exercise in patellar tendinopathy 2,3, supporting the pioneering clinical use by Jill Cook and Craig Purdam4. However, this isn’t quads over fulcrum….
Clinicians need to understand a number of concepts around the use of isometric exercise in tendinopathy. The research has been conducted in the patellar tendon, however clinically we are using with other lower limb tendons. Key considerations include; differential diagnosis (how to pick if the tendon is the source of symptoms), how to remove abusive loading and use loading for analgesia and how / when to progress.
Differential diagnosis
Patellar tendinopathy (pain in the tendon at the front of the knee) occurs in jumping athletes or those that change direction quickly5. It has two hallmark features:
(1) pain remains very localised to the inferior pole (people can point with one finger and it doesn’t move or spread) (Fig. 1), and
(2) dose dependent pain with increasing energy storage tendon load.
A good way of remembering this is that people with patellar tendinopathy can ride a bike without pain because it isn’t energy storage of the patellar tendon but jumping is painful, even though both activities use their quadriceps muscles.
We found differences in the motor responses (termed corticospinal excitability) of people with localized pain compared to people with more diffuse anterior knee pain6. Clinically, we also see that the use of heavy isometrics is better in those that fit the above description of patellar tendinopathy. Those with diffuse anterior knee pain, for example patellofemoral pain, often do not tolerate heavy leg extension holds! This clinical consideration is so important. Remember it is a clinical diagnosis and not an imaging based diagnosis. People with imaging changes in their patellar tendon can have pain driven from another source (such as patellofemoral pain) – we see this often.

How to remove abusive loading
Anything that asks the patellar tendon to store energy and release it is difficult, for example quick lunging and change of direction and jumping. Therefore, athletes may need to reduce these types of activities if their tendon is showing signs of not coping. Signs of not coping can be seen in the response to tendon load 24 hours later. For example if someone plays volleyball and the next day they are no more sore, we would consider this load to be within their capacity7. Whereas, if their pain spiked we would consider the load to be greater than their capacity. This concept is important as is understanding how to improve capacity – find the level of loading that they tolerate and make small increments after you address and any changes. Of course there is a bit more to it that cannot be covered here!
Isometrics for patellar tendinopathy
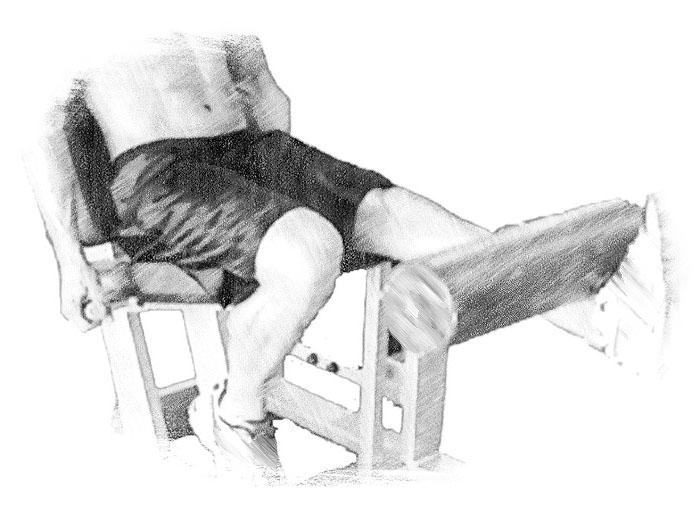
We conducted pilot testing to see what factors were important in using isometrics. It seems for tendons, it needs to be heavy and time under tension is important. We tested lots of combinations and found 5 x 45 seconds (with 2 minutes rest for muscle and central recovery) was effective. It was heavy – 70% of their maximal voluntary quadriceps contraction. Using brain imaging techniques, we were also able to see that isometrics reduced motor inhibition so not only were people in less pain (a lot less pain) they had less inhibition and therefore were 19% stronger! The exercise was conducted on a leg extension machine (Fig. 2). We also completed an in-season trial to show that they can be used in-season to reduce pain and allow participation. We have also completed an isometric research using the Spanish squat belt (see Spanish Squat Exercise) that is currently being prepared for journal submission.
Conclusion
Isometric exercise can be used to reduce tendon pain – immediately and without decline in muscle performance when used as tested. The research is currently in patellar tendinopathy with more to follow. It is important to determine whether the tendon is the source of symptoms or at least determine whether they are likely to respond positively to that approach.
Ebonie Rio has a PhD and a Masters in Sports Physiotherapy, Bachelor Physiotherapy (Hons) and Bachelor of Applied Science. She is currently a post doctoral fellow at La Trobe University and also work at the Victorian Institute of Sport.
Craig Purdam is the Deputy Director of Athlete Services and the Head of Physical Therapies at the Australian Institute of Sport. He has worked as a clinician in elite sport for over 30 years and has been a physiotherapist to five Olympic Games (1984-2000) .
Sean Docking has a PhD and a Bachelor Health Sciences (Hons) and is currently a Post doctoral fellow at La Trobe University. His research interest is in tendon injury.
Jill Cook is a Professor at La Trobe University Sport and Exercise Medicine Centre. Her research interests are in tendon injury, tendon pathology, sports injuries, and musculoskeletal injuries.
References
- Alfredson H, Pietila T, Jonsson P, et al. Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med 1998;26(3):360-6.
- Rio E, Kidgell D, Moseley GL, et al. Tendon neuroplastic training: changing the way we think about tendon rehabilitation: a narrative review. Br J Sports Med 2015.
- Rio E, Kidgell D, Purdam C, et al. Isometric exercise induces analgesia and reduces inhibition in patellar tendinopathy. Br J Sports Med 2015;49(19):1277-83.
- Cook JL, Purdam CR. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. Br J Sports Med 2009;43(6):409-16.
- Malliaras P, Cook J, Purdam C, et al. Patellar Tendinopathy: Clinical Diagnosis, Load Management, and Advice for Challenging Case Presentations. J Orthop Sports Phys Ther 2015:1-33.
- Rio E, Kidgell D, Moseley GL, et al. Elevated corticospinal excitability in patellar tendinopathy compared with other anterior knee pain or no pain. Scand J Med Sci Sports 2015.
- Cook JL, Docking SI. “Rehabilitation will increase the ‘capacity’ of your …insert musculoskeletal tissue here….” Defining ’tissue capacity’: a core concept for clinicians. Br J Sports Med 2015;49(23):1484-5.

Massage Therapy Decreases Cancer-Related Fatigue

Shoulder Decompression Surgery is No More Effective than Sham Surgery
