FFT Case Study: Exposed Leg Fractures
FFT Case Study: Exposed Leg Fractures, by Ron Alexander
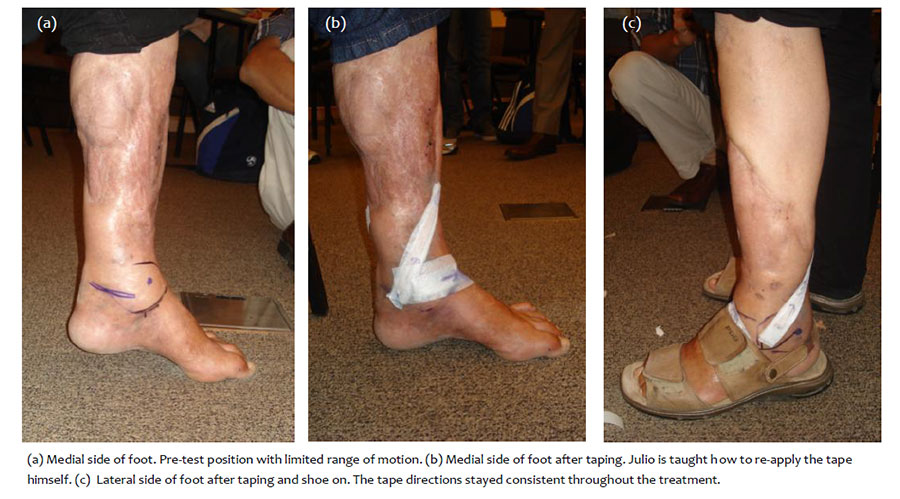
At the Functional Fascial taping (FFT) Workshop in Rio de Janerio, one of the participants, Julio Cesar, a Physiotherapist, suffered 5 exposed fractures as a result of being hit by a truck whilst riding a motorbike 21 years ago. After the accident he was placed in a leg device to lengthen the leg, he then had a surgical fascial release of the Tendo Achilles and the Plantar Fascia.
Before FFT treatment he had a Visual Analogue Scale (VAS) score of 8/10 pain whilst standing and whilst sitting putting weight on the leg and foot. After FFT his VAS score was 2/10. The following day he had no pain standing and walking. He still had limited dorsiflexion which still resulted in a limp, however his gate was better than he had for years. We don’t think dorsiflexion will return to normal due to the amount of damage and surgical procedures. Over subsequent weeks and months Julio self-administered FFT less frequently and then only sporadically. Now, he no longer requires FFT.
Julio’s quality of life has improved dramatically as a result of the tape. At the 12 month follow-up, he reported that he had returned to doing martial arts including competitive fighting, this is after 21 yrs of being unable to participate in any sport due to pain. His surgeon was impressed by this but was unable to explain how the taping could bring about this change. In Julio’s case we were not able to achieve much of an improvement to his range of motion, apart from putting his foot flat on the floor, which was completely achieved the following day. However, this was already a major improvement, his function was much better with significant reduction in pain and he felt optimistic about change in his condition.
The surgeon’s inability to identify how change occurred is a question that still remains unanswered. There are numerous reasons why we experience pain. In Julio’s case, for the first couple of years we can understand it as his condition involved massive trauma, mechanical repair, ongoing mechanical disruption by the process of the lengthening and healing bones and soft tissues, followed by ongoing disrupted biological repair. He followed the standard rehabilitation procedures for someone with this type of injury. This is a complicated pathology that would have many contributing factors, however, in the end, he continued to have pain and it is the residual pain that I viewed from a neuro-fascial perspective.
The application of FFT involves stretching the skin and underlying tissues in a pain-specific direction. One plausible explanation is that the application of rigid tape with tension on the skin could stimulate large-diameter afferent fibres and then modulate nociceptor input (gate control mechanism). In addition to this, stretching the skin in a pain-specific direction with FFT may affect pain perception or it may alter local tissue internal architecture (Ingber 2008) as well as stimulate cutaneous Mechanoreceptors (Grigg 2002). If we view the body from a Biotensegrity principle where living tissue and cells are constructed by discontinuous compression columns (bones) supported and balanced by tension elements (fasciae and connective tissues) resulting in continuous tension (Fuller 1961, Ingber 1998) then FFT may be offering a strong sustained load by tightening components of the mechanical scaffolding of the body. The external force from the tape on the skin may transfer to the underlying tissue and cause multi-laminal sliding movements under the skin, and that could convert into an internal force to evoke different levels and types of mechanoreceptor firing (Chen 2012).
In a practical sense once the tape is applied to the body this potentially creates sustained altered load, the patient is then assisting the treatment by actively moving the affected area and thereby increasing the load provided by the tape . This is custom made for each patient/athlete for an extended and pre-determined period of time. By removing the pain via FFT and having the patient go about normal activity, we are potentially assisting proprioceptively by encouraging muscle firing and restoring normal movement patterns. The patient can now move into this new range, pain free which may assist with the apprehension of pain, elevate mood and re-educate the neuro-muscular system through rehabilitation. In Julio’s case FFT, walking, normal activity and then martial arts was all that was required to reduce his pain, possibly due to the limited dorsiflexion.
We conducted a randomised double-blind placebo-controlled study on FFT for a non-acute non-specific low back pain that demonstrated a significant effect on pain and function with FFT. Although this was conducted on the low back, the same hypothesis of how change occurred can translate to other areas of the body (Chen 2012). This is the process that I used when treating Julio’s condition. FFT has a relative simple objective assessment procedure and tape application that can be fast to do (not in this case study) and is used by any therapist treating neuro-musculoskeletal conditions.
Ron Alexander. Functional Fascial Taping Practitioner [FFTP]. Director/Founder of the Functional Fascial Taping Institute Melbourne, Australia. Co-Investigator Randomised Double Blind Placebo Controlled Trial of FFT for Non-Specific Low Back Pain [PhD] Deakin University Melbourne, Australia. Awarded the Lady Southey Scholarship for Excellence from the Australian Ballet Foundation. Presented FFT to the International Olympic Committee World Congress, the Royal College of Surgeons UK. Fifth, Sixth and Eighth Interdisciplinary World Congress on Low Back & Pelvic Pain and the Fascia Research Congress 2007 including an FFT workshop at the FRC in 2012. Ron teaches FFT in Sydney and Melbourne in April 2016. Details here.
References
Alexander R. 2014. Functional Fascial Taping and Research. Terra Rosa e-magazine, No. 14.July. pp 24-29.Chen SM, Alexander R, Sing KL,Cook J. 2012. Efficacy of Functional Fascial Taping on Pain and Function in Patients with Non-Specific Low Back Pain: A Randomised Controlled Trial. Pub Clin Re-hab Oct 2012 Vol 26, No. 10. 924-933.
Chen SM, Alexander R, Sing KL,Cook J. 2012. Efficacy of Functional Fascial Taping on Pain and Function in Patients with Non-Specific Low Back Pain: A Randomised Controlled Trial. Pub Clin Re-hab Oct 2012 Vol 26, No. 10. 924-933.
Chen SM. 2012. FFT PhD Thesis. Neurophysiology of the Cutaneous Mechanoreceptors. Deakin University, Supervised by Professor Jill Cook.
Grigg P and Del Prete Z. 2002.Stretch sensitivity of cutaneous afferent neurons. Behav Brain Res; 135: 35–41.
Ingber DE. 2008. Tensegrity-based mechanosensing from macro to micro. Prog Biophys Mol Biol; 97: 163–179.
Macgregor K, Gerlach S, Mellor R, et al. 2005. Cutaneous stimulationfrom patella tape causes a differential increase in vasti muscle activity in people with patellofemoral pain. J Orthopaed Res; 23: 351–358.