Remote stretching based on myofascial meridians is as effective as local stretching
According to a study published in the Journal of Sports Science, “remote” stretching the lower limb is as effective as local neck stretching in cervical spine range of motion (ROM) improvement. This could have an interesting application for patients for whom stretching of the neck is contraindicated.
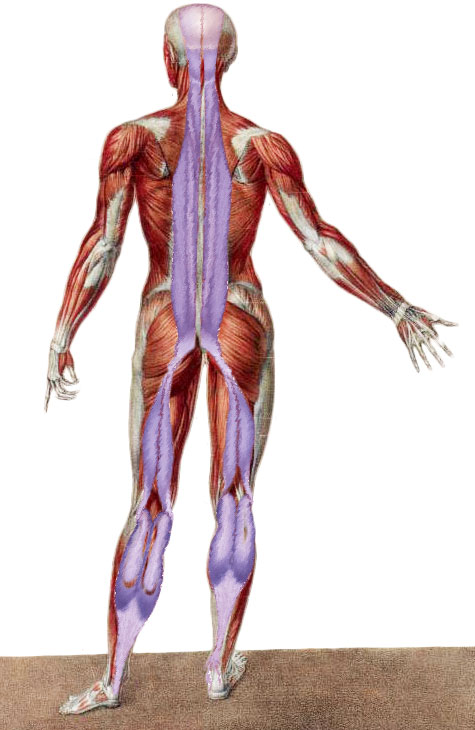
The results of this study validate the presence of the “superficial back line” myofascial meridian (plantar fascia, Achilles tendon, gastrocnemius, hamstrings, sacrotuberous ligament, thoracolumbar fascia, erector spinae, occipitalis/galea aponeurotica/frontalis). Plantar massage can increase hamstring extensibility, while stretching the gastrocnemius and hamstrings can increase cervical spine mobility in the sagittal plane. Now, researchers from Goethe University in Germany, led by Dr. Jan Wilke, attempted to answer the question whether remote stretching on the myofascial meridian is as effective as local stretching at some point along its length.
The study recruited 63 healthy participants (36 ± 13 years) whom were randomly assigned to one of three groups: remote lower limb stretching (LLS), local cervical spine stretching (CSS) or inactive control (CON). Maximal cervical spine ROM in the sagittal, transverse, and frontal planes was assessed using ultrasound prior (M1), immediately post (M2), and 5 minutes following intervention (M3).
The results showed that, with one exception (cervical spine rotation after CSS at M2), both lower limb and cervical stretching increased cervical ROM compared to the control group in all movement planes and at all measurements. Importantly, no statistical difference was found between local and remote stretching. However, the attained effects do not seem to be direction-specific, in other words, do not seem to be related to the plane of movement of the stretch. The authors concluded that lower limb stretching based on myofascial meridians induces similar short-term improvements in cervical spine ROM as local neck stretching.
The authors consider 3 possible underlying mechanisms:
(1) neurologic adaptation, which is in accord with a common knowledge that stretching musculature in one region of the body can affect central nervous system mediated baseline muscle tone elsewhere in the body, both ipsilaterally and contralaterally,
(2) myofascial force transmission, i.e., transmission between muscle and fibrous connective tissues along a myofascial continuity (in this case the superficial back line myofascial meridian),
(3) peripheral neural tissue force transmission, because peripheral nerves cross multiple joints in a similar manner to myofascial chains, they may act as force transmitters.
The authors favour the neurologic adaptation and myofascial force transmission mechanisms; the peripheral neural tissue force transmission mechanism was discounted because peripheral nerves do not have continuity from the leg to the head. Further, given that the effects were seen along the superficial back line myofascial meridian, the myofascial force transmission mechanism seems particularly promising.
Nevertheless, this speculation still needs further research clarification. The authors also questioned the reciprocity of the stretching effects. While stretching the lower limb has now been shown to cause remote effects in the cranial direction, the reciprocal effect is unclear. In other words, would cervical stretching have an effect in the caudal/inferior direction at the lower limbs? A past study did not observe a change in the ankle ROM when flexing the cervical spine. We look forward to future studies to clarify the mechanism(s) that allow remote stretching to increase ROM and flexibility elsewhere in the body.