The evidence of Anatomy Trains Myofascial Meridians
They looked for relevant human anatomical dissection articles published between 1900 and December 2014 in scientific publication databases. The authors appraised peer-reviewed anatomical dissection studies that reported morphological continuity between the muscular components of the meridians. In addition, papers on general anatomy of the corresponding body region were also searched. A continuity between two muscles was only documented if two independent investigators agreed that it was clearly reported. Also, two independent investigators rated methodological quality of included studies by means of an assessment tool called QUACS (Quality Appraisal for Cadaveric Studies). The review identified 6589 articles. Of these, only 62 papers met the inclusion criteria.
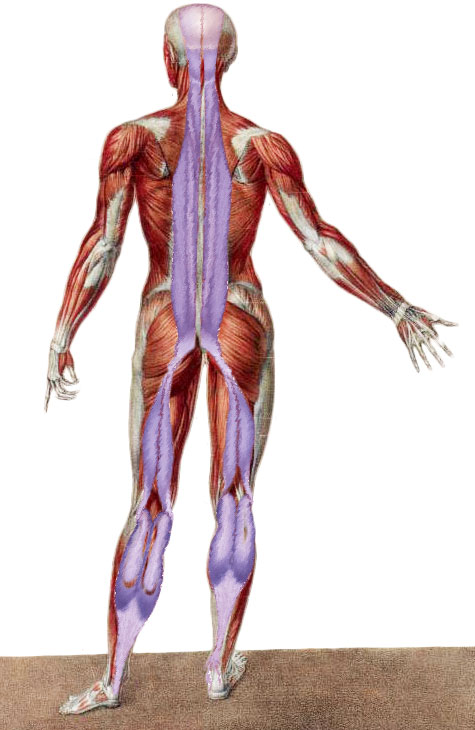
The review suggests strong evidence for the existence of three myofascial meridians: the superficial back line (all three transitions verified, based on 14 studies), the back functional line (all three transitions verified, 8 studies) and the front functional line (both transitions verified, 6 studies). Moderate to strong evidence is available for parts of the spiral line (five of nine verified transitions, 21 studies) and the lateral line (two of five verified transitions, 10 studies).
However no evidence exists for the superficial front line (no verified transition, 7 studies). There is no reported structural connection between the rectus femoris muscle and rectus abdominis. Also, sternalis, which is suggested to be the cranial continuation of rectus abdominis, exists only in a small percentage of the population. Even if present, it does not fuse consistently with the rectus abdominis.
The authors suggested that the practical relevance is twofold. First, the existence of the myofascial meridians might help to explain the phenomenon of referred pain. For example, myofascial trigger points of the calf have been shown to elicit pain that radiates to the sole of the foot and to the dorsal thigh. A second aspect relates to therapy and training of the musculoskeletal system. Treatment according to myofascial meridians could be effective in reducing back pain. Several studies have shown that low back pain patients display reduced hamstring flexibility. Overload injuries in competitive sports represent another entity of pathologies which possibly occur due to the presence of myofascial meridians. Recent studies indicate that tightness of the gastrocnemius and the hamstrings are associated with plantar fasciitis. Groin pain or athletic pubalgia is suggested to be provoked by a tight adductor longus and a weak rectus abdominis. Strain transmission along meridians would both open a new frontier for the understanding of referred pain and provide a rationale for the development of more holistic treatment approaches. The study was published in the August 2015 issue of Archives of Physical Medicine and Rehabilitation.
A couple of studies also look at the functional relationship of the superficial back line. In a study from the University of the West of England, the researchers deemed it is necessary to do an experiment as “To date there is no evidence to support the effect of bilateral self myofascial release on the plantar aspect of the feet to increase hamstring and lumbar spine flexibility.” Twenty four healthy volunteers underwent screening to exclude hypermobility and were randomly allocated to an intervention of self myofascial release (SMR) or control group (no therapy). Baseline and post-intervention flexibility were assessed by a sit-and-reach test (SRT). The results showed that there was a significant increase in the intervention SRT outcome measurements compared to the control group. And thus concluded that “An immediate clinical benefit of SMR on the flexibility of the hamstrings and lumbar spine was indicated”.
A second study from the Republic of Korea, investigated if the flexibility of the hamstring can be increased by targeting the suboccipital muscles. The study used two techniques SMI (Suboccipital Myofascial Induction), where a therapist applied a myofacial release on the occipital muscles, and SMR (Self Myofascial Release) where the patient used a triangle-shaped pillow placed under the patient’s occiput to apply pressure to the suboccipital area. Fifty persons with short hamstrings participated in this research, the subjects were allocated either the SMI or SMR. The results showed that in the SMI group, finger-floor distance (FFD), straight leg raise (SLR), and popliteal angle (PA) were significantly changed after 5 minustes of intervention. In the SMR group, there was a significant change in SLR after the intervention. The authors concluded that the application of both techniques to patients with short hamstrings resulted in immediate increases in the flexibility of the hamstring.


