Functional impairment following DOMS is related to mechanosensitive nociceptors
Delayed-onset muscle soreness (DOMS) refers to pain and discomfort in people after participating in exercise and physical activities. This mechanically induced microtrauma results in muscle soreness associated with pain and weakness. The dull pain and discomfort are usually felt 6 to 12 hours and peaking 48 to 72 hours after exercise.
There is still a debate about why this pathophysiologic response mediates pain. There is no consensus regarding the origin of pain.
Some researchers suggest muscular fascia to cause pain, while others showed the presence of cutaneous allodynia. While muscular fascia could induce local nociceptors (peripheral sensitivity), pain could be a result of increased spinal sensitivity. Also, the breakdown products of the impaired muscle tissue could excite nociceptors.
Muscle nociception is supposed to involve high-threshold mechanosensitive receptors (HTM, on C and Aδ-fibres). These HTM units are activated when a certain pressure threshold is exceeded. The receptors are first stimulated by chemical mediators and then activated by the increased interstitial pressure caused by the intramuscular swelling due to DOMS-related oedema. Once activated, the signal is transduced by the activation of a variety of voltage-gated ion channels that convey the signal to the dorsal horn. The signal is mediated to the CNS, which leads to the processing of nociceptive messages. In persistent pain, the peripheral sensitisation could alter the properties of peripheral nerves. This pain from inflammation-associated changes the chemical environment of the nerve fibres. The changes could further enhance the excitability of the nociceptor and amplify the neurogenic inflammatory response.
A study from Frankfurt, Germany examined the effect of these mechanical thresholds on DOMS. Twenty healthy participants were induced for DOMS on the non-dominant arm. Mechanical pain thresholds were then measured at baseline, 1,2, and 3 days after induction. The target muscle is the biceps.
The results found that
- DOMS reduced the pressure pain threshold (PPT) at 48 hours. This is accompanied by the decrease in the maximum isometric voluntary force (MIVF).
- Subjective pain was felt until 48 hours, however the PPT was still present after 72 hours.
- The change in PPT (before and after DOMS) is highly related to the change in pain intensity or the sensitivity of PPT.
- Change in maximum isometric voluntary force is related to the change in PPT.
The study showed that PPT was the only mechanical pain measurement that correlated significantly with the perceived participative muscle pain intensity. PPT seems to be the most significant predictor of pain, suggesting this is an intramuscular pain origin.
Thus, the authors concluded that functional impairment following DOMS is related to the increased excitability of high-threshold mechanosensitive nociceptors.
The authors further concluded that PPT was the most valid parameter that can predict dysfunction. PPT, rather than pain intensity, should be considered a possible marker indicating the athletes’ potential risk of injury.
Massage therapy that mechanically stimulates nerve and fascia may modulating these mechanosensitive receptors which can lead to pain reduction or function recoveries. Normalising the pain sensitivity or threshold could be another mechanism that could be considered.
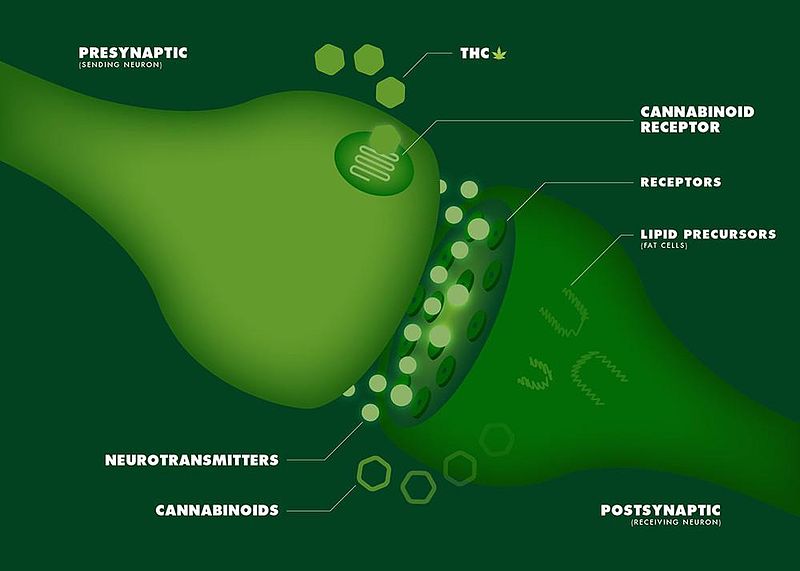
Expression of the endocannabinoid receptors in human fascial tissue
Muscle Imbalance and Overuse in Elite Junior Short-Track Speed Skaters
