Ron Alexander on Functional Fascial Taping® and Research
Can you explain how the research project on Functional Fascial Taping (FFT) came about?
I have always been interested in being involved in a research project as have always been interested in how and why things work. Someone said to me years ago that you study to do clinical work and then you continue to learn through doing this work, however, it’s also important to further your understanding through post graduate courses, reading and discussing ideas with peers. Taking part in a research project is a process that allowed me to combine my practical experience and theoretical knowledge and to ask questions about FFT. Research provides the opportunity to test these ideas under controlled conditions. This scientifically adds validity to what you do, whilst increasing your own depth of understanding. Then you have the ability to implement the results into your clinical practice and share this knowledge. This process leads to further clinical observation and questions, and the cycle continues. This constant process of enquiry and testing is what I really enjoy about research.
I had discussed the possibility of conducting a research project on FFT with Dr Jill Cook, Head of the Musculoskeletal Research Unit, at Deakin University. As a result of our discussions Dr Cook referred the following patient to me as a test case to determine if FFT could assist a long standing chronic non-specific low back pain patient.
The following provides a brief clinical overview of this patient, for a more detailed explanation follow the link. The patient had a history of back pain for 14 years. She had 2 laminectomies for disc decompression. These procedures were 18 months apart, both were unsuccessful and she continued to have pain for the next 2 years. Three months prior to the commencement of the FFT treatment, a trunk flexion test showed trunk flexion to be 15°. The patient was given three treatments over a one week period and was able to achieve full flexion. The tape was worn for a further 5 weeks and she was weaned off the tape during this period. The patient made a full recovery, experiencing full range of movement and the total absence of pain.
Her final progress was followed up at 3 years with no pain and full range. This successful case study indicated to Dr Cook that a RCT (randomized control trial) on FFT was warranted in order to determine if this result could be replicated with a larger sample size. It had taken me many years of trial and error to get to this point. Dr Cook sourced a Deakin University PhD Physiotherapy student, Shu-Mei Chen who was on scholarship from Kaohsiung Medical University Hospital, Taiwan to conduct the trial. I then submitted the case study for review by the Scientific Committee for the first Fascia Research Congress (FRC) at Harvard and it was accepted as a poster* presentation (Alexander, 2008a), available here. Presenting this at the Congress was a great experience as it gives the presenters of posters the ability to talk about studies to delegates and other presenters.
Case studies have a role to play in clinical practice and research. Case studies provide the reader with the ability to gain a broader understanding of clinical assessments, treatments and outcomes, and thereby create informed discussion amongst peers. Although the case studies are in themselves not strong evidence for the efficacy of a treatment they can form the basis of research topics and RCTs to test the validity of a treatment scientifically.

Figure 1. Taping the foot.
You presented two posters at the first FRC in Boston. What was the topic of the second poster?
The second poster focused on the results of two real time ultra-sound (RTU) investigations that we conducted into the effect of tension/load from tape (Alexander, 2008b) . The first RTU was filmed at the Australian Institute of Sport. The procedure involved applying the tape to the quadriceps. We observed the region before and after the application of tape with active knee flexion and extension (FE), to ascertain change. Interestingly we also filmed the application of the tape, without knee movement, in order to observe the presence of load being applied. The tape direction was longitudinal to the thigh and was ½ width of the standard 38mm wide, which makes it tighter. This comes about because force over area equals pressure and in this case, the pressure is tension. So if we decrease the width of rigid tape, we increase the force and therefore more tension is possible. When the tape was applied the subcutaneous tissue including the superficial fascia moved in the direction of the tape. The deep fascia and the muscles below at 3cm deep, moved in the opposite direction. The effect was more than likely deeper, however, the RTU was not calibrated to view the thigh at any greater depth than 3cm. On this occasion we were in fact able to blame the equipment. The tissues and the Retinacula Cutis are held in a new position and muscle activation post-application was completely different from pre-application. See the “RTU” section below for footage. Many therapists who have viewed the RTU are of the opinion that we are potentially viewing Myofascial Release inside the body, for the first time.
The other RTU was conducted in Perth with a very skilled Musculoskeletal Physiotherapist Felicity Kermode who lectures on RTU in various countries. We investigated the Abdominal region using the apex of Transverse Abdominis (TrA) as a reference point to observe if a movement was possible from tape. For a more detailed explanation See “RTU”. We applied tape to the Contralateral side of the body on the Thoracolumbar Fascia (TLF). The tape direction was from Lateral to Medial using the FFT gathering technique. We thought we may see an effect because the TLF is connected to the TrA. The result was really interesting because the TrA moved in the direction of the tape, however what we didn’t expect and what happened was that the whole abdominal cavity moved, the RTU measured 0.94cm displacement and was in the direction of the tape. The subject remained seated for a period of time and the tissues were held with sustained load in this new position. This observation may lead to new developments in Visceral Manipulation.
Have there been any other RTU investigations conducted in relation to FFT?
We have conducted many more RTU observations and each time the Subcutaneous Tissue (SCT) moves in the direction of the tape. So we can say with confidence that the SCT and the Superficial Fascia Tissue Layer (SFTL) move in the direction of the tape and it has a controlling or stabilizing effect to those layers.
We have observed the same movement of tissues in a distant region. For example, we have applied tape to the proximal forearm, whilst observing with the transducer at the wrist and we observed the SCT and the SFTL move in the direction of the tape and the deep structures moved in the opposite direction and this change was on the opposite side of the body to where we were applying the tape. One possible explanation for this, if we think of the Biotensegrity principle where living tissue and cells are constructed by discontinuous compression columns supported and balanced by tension elements resulting in continuous tension (Fuller 1961, Ingber 1998, Levin 2002) then FFT may be offering a strong load by tightening components of the mechanical scaffolding of the body. It may alter the skin and/or remodel the internal architecture of the connective tissue (Ingber 2008, Langevin 2010). These tissues are heavily innervated with mechanoreceptors and potentially change the neural input by stimulating large-diameter afferent fibres and then modulate nociceptor input.
Another part of our study on FFT also included an RTU investigation on 23 asymptomatic subjects, this was filmed with Deluca J, Senior Musculoskeletal Sonographer at Latrobe University Medical Centre. We investigated motion analysis, from standing position, moving into truck flexion to 65°. The transducer was kept in constant contact with the skin as the participant performed flexion. In all cases apart from one, the SCT and the SFTL moved independently from the deeper structures and then at some point in range they moved together. The case that did not follow this pattern had the complete opposite reaction in that the tissue layers worked together and then at a point in flexion they worked independently. In an attempt to find out why this occurred we questioned the subject and found out that she was doing regular Pilates, which may have given her better core recruitment and naturally wanting to bend from the hips, however, when asked to bend from the low back she demonstrated a similar pattern of the tissues sliding independently of each other first and then together. The concept of tissues sliding on one another has been around for some time for muscles, tendons and mechanical interfaces. This concept was later applied to the superficial tissues and other structures from the great work by Plastic Surgeon Dr Guimberteau JC and his famous DVD “Strolling under the skin”, which provides an exquisite demonstration of morphing fascial tissues in patients, ongoing surgical procedures and returning back to the original configuration when the tissue is released.

Figure 2. Taping the hip.
Why apply FFT when everything goes back to the way it was?
By decreasing pain and assisting function, we return a patient to normal movement patterns. This is a key element in the treatment plan because FFT is holding the body in a pain free state for an extended period of time determined by us. Potentially, the tape provides proprioceptive muscle activation and creates a decrease in fear avoidance behaviour, as patients are encouraged move into a previously painful position without pain. This state allows patients to perform simple or complex activities depending on the presenting history. Sometimes just having the patient go about normal activity can be enough for them to achieve recovery. However this depends on the duration, nature and severity of symptoms and quite often additional rehabilitation advice is required. This allows the therapist to more accurately address the signs and symptoms of the musculoskeletal condition.
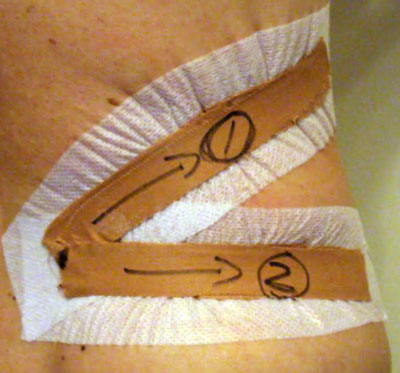
The tape is applied in the direction of optimal ease, which is variable and this is determined from the FFT Assessment procedure. However clinically for years I have observed that sometimes when you apply FFT, the tape direction that relieves pain can sometimes be in the direction or the opposite direction of movement that you are trying to increase. Tape is applied with almost maximum tension by the use of a gathering technique to take the skin and tissue slack up, in the direction you are trying to increase (See Figure 1). Wouldn’t this logically decrease range of motion?
However in over 95% of cases what we see is that it actually increases range of motion (ROM). There are some specifics to this application in some regions and I know that this sounds counterintuitive, nevertheless we see this take place in most regions in the body and I find this extremely interesting. I have observed this result thousands of times, firstly with the dancers at the Australian Ballet, then later with athletes and patients. I have taught this technique to thousands of therapists who have observed the same outcome. I have thought for many years that superficial structures could be working independently of the structures below as well as potentially changing neural input. This thinking is supported by a cadaver dissection of the SCT and the SFTL conducted by Gil Hedley. This was the first time a dissection of this type had ever been conducted and recorded. Hedley removed the entire skin layer. He then sliced through the Reticular Cutis to remove the SCT and the SFTL from the Deep Fascia. Hedley also moved the layers on each other to demonstrate the amount of available movement. Put simply in practical terms, you can distract your skin and underlying tissue with strong sustained load, whilst moving your arm. As therapists we do this all the time when performing myofascial release with active motion.
We conducted another experiment to determine how far the skin and underlying tissue can move in the low back. This was another part of Chen’s PhD. In this experiment, we applied tape in a lateral direction 4cm above and 4cm laterally away from the posterior superior iliac spine (PSIS). We then used the PSIS as a reference point and graphed the body over the hip. The result was that both the skin and underlying tissue had the ability to move up to 2.4cm. This test was undertaken on asyptomatic subjects, we have not as yet tested subjects with super hypermobile tissue, such as Ehlers-Danlos syndrome. The results would also vary in different areas such as over the tibia.
When applying FFT the assessment procedure and tape application, one end of the tape is placed directly on the pain site, therefore, load is going away from this point. Taping this way is unique to FFT. The tape is applied with a strong loading force. The start point could be called point A, the other end of the tape where a resultant reactive force would be created, called point B. Both these ends pull the skin and underlying tissue towards the centre of the tape, point C. In the centre, there would be a balance between these two forces (See Figures 2 & 3). According to the tensegrity principle, external force on the skin can transfer to the underlying tissue and cause multi-laminal sliding movement under the skin, and that could convert into an internal force to evoke different levels and types of mechanoreceptor firing (Chen 2012). The load from both ends pulling into the centre is consistent with Newton’s 3rd law, where every action has an equal and opposite reaction. It’s nice when the physical laws of motion appear to support many years of clinical observation. This concept potentially will lead to new insights into Mechanotransduction and Mechanotherapies.
Pain can come from numerous sources in the body and the effect of applying rigid strapping tape on the body is multidimensional. The principle and application of FFT is different to other rigid taping techniques (RTT) that have been shown to be effective in decreasing pain. My observations of the effect of FFT on the body does not take away from current theories regarding RTT. It is looking at taping from a different perspective.

Figure 3. Taping the knee.
How can I get involved with a research project?
There are various levels of research, if you are looking at robust RCTs, then it is a process that requires a certain level of academic expertise and a different skill set, whereby you will need to work cooperatively with relevant departments within universities. RCTs are normally conducted at PhD level, although there are exceptions to this. A clinician’s involvement can take on many forms and levels, and can lead to higher qualifications if that is part of your goal. In my case, I took on the role of co-investigator for three of the trials. You will need to contact the relevant department of universities to discuss your proposal. If they are interested, the professor who will oversee the project, should have a list of students who may be interested in undertaking the research.
The depth of understanding that comes from being involved with a rigorous scientific trial, is helped by reading scientific literature and undertaking clinical work. If your study supports what you are investigating and you have a great team then they should have the ability to produce a good publication that will be published in a respected journal with a wide readership. This in turn, supports our industry.
Have you got any tips?
RCTs do take a while. The processes involved are research design, systematic review, ethics application, clinical trial, data collection, publication and thesis. It’s good to remember that the research team will be focused on the method and the processes involved in the project. The subject or technique in the study, is only one part of the project. The best research is done in collaboration and the ability to compromise is important, which can be challenging at times. Also the amount of detail required in robust trials is incredible resulting in a very lengthy process, patience is required and the ability to not lose sight of the bigger picture of getting a study completed and published. It might also come as a surprise that no one does research in today’s world without a publication in mind.
It may also be worth keeping in mind that the investigation may not be exactly the scope that you had intended. I have found that sometimes people try to either support something too hard or want to look at too many variables and this stops the study from ever getting off the ground. It may be better to do a more limited study and then do a follow up study at a later date. Having a study published in an international scientific journal gives credibility which can make it easier the second time around for your team. My last tip is to believe in yourself, the technique and your team as these elements will see you through when the going gets tough. The knowledge that I have personally gained through the research process has been invaluable. Lastly, good luck and remember, nothing ventured nothing gained!
Ron Alexander teaches FFT regularly in Australia and all over the world. Fore more information on FFT workshops in Australia, visit here.
References
*Posters. Fascia Research Congress Boston, MA, October 4-5, 2007. The Conference Center, Harvard Medical School. www.fasciacongress.org. Full colour version online download at www.fft.net.au
Chen SM, Alexander R, Lo SK, Cook J. 2012 Efficacy of Functional Fascial Taping on Pain and Function in Patients with Non-Specific Low Back Pain: A Randomised Double Blind Placebo Controlled Trial. Clinical Rehabilitation Vol 26, No. 10. 924-933.
#Chen SM. 2012. FFT Thesis. Neurophysiology of the Cutaneous Mechanoreceptors. Deakin University, Supervised by Jill Cook.
Alexander R. 2008a. Functional Fascial Taping for Lower back pain: A Case Report. Journal of Bodywork and Movement Therapies. Volume 12, July 2008, Pages 263-264.
Alexander R. 2008b. Functional Fascial Taping Real Time Ultrasound Investigation. Journal of Bodywork and Movement Therapies. Volume 11, April 2008, Pages 390 – 391.
Fuller B. 1961. Tensegrity. Portfolio Artnews Annu, 4, 112-127.
Levin S. The tensegrity-truss as a model for spine mechanics: Biotensegrity Journal of Mechanics in Medicine and Biology. 2002 vol. 2, #3&4, 375-388.
Ingber D. 1998. The architecture of life. Scientific America.
Ingber D. 2008. Tensegrity-based mechanosensing from macro to micro. Prog Biophys Mol Biol. 97:163-179.
Langevin HM, Storch KN, Snapp RR, et al. 2010. Tissue stretch induces nuclear remodeling in connective tissue fibroblasts. Histochem Cell Biol; 133: 405–415.
Real Time Ultrasound (RTU) of Taping Effect
The procedure involved applying the tape to the quadriceps. All 3 movie files are 5 second shots and repeated. The hip is right of screen in all shots. The tape width is ½ width of the standard 38mm wide. The transducer is longitudinal muscle fibre direction, in a Mid Saggital line to the Quadriceps Muscle. The small dots on the left of screen are the RTU measuring cm’s deep. 3cm’s deep is shown and a depth of approximately 2mm, we can observe the Subcutaneous tissue layer and the Superficial Fascia layer. Approximately 3mm the Deep Fascia. Greater than 4mm deep, the Muscles. One piece of tape applied, the standard tape application is 3 layers which are tighter each application.
1) Before Flexion and Extension, No Tape.
The first is shot is pre-tape observation under normal conditions with active knee flexion and extension. Observe the amount of movement in the Superficial Fascia layer and the muscle tissues relationship to each other.
2) Presence of tape being applied with tension (load).
The application of one piece tape with tension, without knee movement, in order to observe the presence of load being applied. The deep fascia and the muscles below are moving in the opposite direction at 3cm’s deep.
3) With tape on the body with active Flexion and Extension.
The tissues are held in new position, with load. The muscle activation post application is completely different from pre-application. We can observe virtually immobilisation of the Subcutaneous tissue layer and Superficial Fascia layer. Observe change taking place at the Deep Fascia, Retinacula Cutis and the muscle activity is different from the first RTU.
Real Time Ultra-Sound Investigation of the left Abdominal region.
The shot is 7.5cm deep, 1 cm markers are shown left of screen. We can observe the skin and the Subcutaneous Tissue layer. First muscle External Oblique followed by Internal Oblique, Transverse Abdominis (TrA) and then the Abdominal cavity.
The apex of the TrA is used as a reference point. A little black digital marker can be seen near the center of screen. This is a part of the RTU machine’s measuring tool. At the right of screen you can see +DIST 0.02cm displayed. It should be 0.00, so we need to subtract 0.02 of at the end. The digital maker is going to be moved manually, to follow any potential movement of the apex of the TrA. We applied tape to the Contra Lateral side of the body. The tape were applied to the Thoracolumbar Fascia from Lateral to Medial using the FFT gathering technique, with 4 pieces of rigid tape. The white areas shown in the body are the Connective Tissues and the Fascia being highlighted. The TrA moves to the right of screen and then is measured. What we observe is that the entire Abdominal region moves in the direction of the tape. The RTU displays 0.96cm however taking off the 0.02, it shows 0.94cm in the direction of the tape. There is no skin or subcutaneous tissue movement which possibly is because a standoff is not used (standoff allows the skin to move) and more than likely the transducer is blocking the tissue.
You may need to watch a couple of times to make out the RTU digital maker and Connective Tissue movement.
Physical Activity: A Proven Antidote for Depression, Anxiety, and Distress

ITB: Don’t let one study deter you from work on this area —Art Riggs
