Sacral neurons reassigned to sympathetic
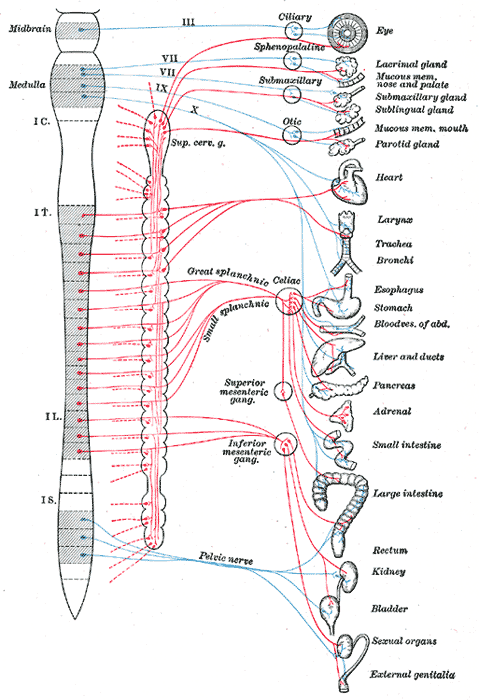
The autonomic nervous system regulates the function of internal organs such as the gut. It is divided into sympathetic and parasympathetic subdivisions, the yin and yang control mechanism for stress responses (fight or flight) and homeostasis (rest and digest). The parasympathetic and sympathetic tend to work antagonistically. Sacral autonomic outflow is traditionally assigned to the parasympathetic division of the visceral nervous system—as part of the “cranio-sacral outflow”
In a recent publication in Science, Isabel Espinosa–Medina and colleagues from France used anatomical and modern molecular analyses to show that the autonomic motor neurons in the sacral cord share similar characteristics with the sympathetic motor neurons in the thoracic cord and not with the parasympathetic motor neurons in the hindbrain.
Dr Peggy Mason, a Professor of Neurobiology at University of Chicago wrote on her blog :
“The crux of the change implied by reclassifying sacral autonomic motor neurons as sympathetic is that two functions, hitherto classified as parasympathetic, are in fact sympathetically controlled: Voiding (both urine and feces), and Sexual arousal (including erection in males)
In sum, spinal autonomic outflow belongs to a single branch of the autonomic nervous system, that which we call sympathetic. The functions of this unified sympathetic aka spinal autonomic system are many “f”-s: fleeing , freezing, fighting, f-cking (excuse me), and two “p”-s: peeing and pooping.”
Kevin Patton, from the A&P Professor website, wrote: “In a nutshell, the new model stipulates that the outflow (efferent pathways) are divided into a cranial division and spinal division— NOT the craniosacral and thoracolumbar divisions that we learned (and that exist in all A&P textbooks):
Current model:
- Craniosacral division (parasympathetic outflow)
- Thoracolumbar division (sympathetic outflow)
New model:
- Cranial division (parasympathetic outflow)
- Spinal division (sympathetic outflow).
Comments by Til Luchau
We were totally wrong: the sacral autonomic outflow is sympathetic. We all learned that the sacral plexus were the second major centre of parasympathetic neuron concentration (after the vagus nerve), but a paper by published in the Nov 18, 2016 issue of Science has me fairly convinced that’s not the case.
If true, this reclassification means a lot of our ideas about the role of sacral approaches to calming the autonomic nervous system (ANS) may need fairly major revisions. This has implication on approaches that include Ida Rolf’s pelvic lift technique, craniosacral therapy, and trauma-informed approaches such as TRE and Porges’ Polyvagal Theory, to name a few. (And, the last chapter of my second Advanced Myofascial Techniques book. Darn; it just came out. But it’s still a cool discovery.)
The Big Question: Does this change how we should work? I’ll leave the details of the reclassification to the sources below, but as other newly emerging disruptive explanations (such as the changing views of pain and nociception; the debates about the importance or unimportance of biomechanics, the questions about the plausibility of tissue change explanations for the results we see), the key question is, how does this change what we do in the practice room?
If we could correct for confirmation bias (and we can’t, at least not by ourselves), we could say that if the old methods work, then maybe we just need to explain them differently. If people seem to get calmer with a pelvic lift technique, for instance, then it is presumably doing what we want it to, even if we need to update our theory about why it seems to work. A rose by any other name, after all, smells just as sweet.
Or so they say. But since we’re all prone to look for the results we expect to see, I wonder what will happen if we start imagining that we’re affecting sympathetic function (instead of parasympathetic function) with our pelvic lifts, sacral holds, etc.? Are there new possibilities that this shift opens up? For instance, can we up-regulate via a pelvic lift, as well as down-regulate?
The only little niggle I still have is that it seems the reclassification done by genetic and phenotyping, rather than by observing the actual functional effects of the neurons involved. In other words, I don’t see any evidence that the actual effects were considered, just their origin and structure. But as Peggy Mason suggests in her fun video, it seems that the neurons’ function wasn’t the main way these structures were classified as sympathetic or parasympathetic in the first place; that it was always anatomy, rather than function, that gave them their classification . Here is the YouTube short from Prof. Peggy Mason https://youtu.be/uV0RRlazx-Y
Comments by David Lesondak
Overall, I think it’s great that we can still find out that we got something so basic so wrong, and for so many years.
It gives me great hope that this discovery will open more minds to question the dogmas of science, which can sometimes close the door to innovation. And frankly it makes a kind of sense, for example I could never wrap my head around the idea that sexual arousal and responses were parasympathetic activities. And I am sure that we will discover part of what’s al at play here will also involve the enteric nervous system.
As far as my practice and treatment is concerned, this discovery isn’t going to effect it. It was drilled into me for years that you end every treatment with subocciptal work, followed by a series of “pelvic lifts” (essentially long, slow traction along the lumbar spine, with your patient supine and your hand underneath). This was stimulate a parasympathetic response.
I stopped doing that years ago. No more pelvic lifts. No specific reason, except people seemed quite sufficiently mellowed out after treating their suboccipitals and so anything else seemed intrusive and unnecessary. And omitting it didn’t seem to have any effect on the outcome. Now when I do psoas treatments I usually do lumbar traction for the sake of reciprocal stimulation, but that’s about it these days.
So, in summary, I am quite glad the science has now given me a rationale for something I quit doing years ago!

Research Update June 2017
