The anatomical and functional relation between gluteus maximus and fascia lata

Gluteus Maximus (GM) is usually described as the largest muscle of the human body having various functions. Some studies have identified GM as having the largest capacity for external rotation of the hip thanks to its insertion into the linea aspera of the femoral bone. Others consider fibres from the more cranial sites of origin primarily end in a thick laminar tendon that inserts on the iliotibial tract. The activity of the cranial portion is ‘considerable’ increases during jogging and running. Other studies have identified a role in hip flexion due to the insertion of the GM in the iliotibial tract. Meanwhile another study said the most important insertion of GM is the iliotibial band.
There is not full agreement regarding the distal insertions of the gluteus maximus muscle (GM), particularly the insertions into the iliotibial band and lateral intermuscular septum. A study led by Antonio Stecco from the University of Padova, Italy, published in Journal of Bodywork & Movement Therapies, studied 6 cadavers, 4 males and 2 females, mean age 69 yr, dissected to evaluate the insertions of the GM into the iliotibial band, fascia lata, lateral intermuscular septum and femur.
They found that the distal insertions of the GM are more fascial then osseous. The iliotibial band is a reinforcement of the fascia lata and cannot be separated from it. Its inner side is in continuity with the lateral intermuscular septum, which divides the quadriceps from the hamstring. In all subjects, the gluteus maximus presented a major insertion into the fascia lata, so large that the iliotibial tract could be considered a tendon of insertion of the gluteus maximus. Gluteus maximus muscle transmits its force not only to the linea aspera of the femur, but also to a wider surface composed of the fascia lata, the iliotibial tract (ITT) and the lateral intermuscular septum.
The contraction of the gluteus maximus muscle always affects the ITT and all of the fascia lata, which explains why a hypertonicity of this muscle could be responsible for an iliotibial band syndrome (ITBS) or, more generally, knee pain. When a therapist encounters a patient with an ITBS or a knee pain, we need to check the gluteus maximus and the tensor fasciae latae muscles. This is confirmed by the study of Chen et al. (2006) who demonstrated that gluteal contracture causes a posteromedial displacement of the ITT, and that the resolution of the ITBS can be achieved only when the biomechanics of hip muscles are properly addressed.
The gluteus maximus muscle also has an important insertion into the thoracolumbar fascia, as shown by Andry Vleeming. He showed that the gluteus maximus is linked anatomically to the lumbar paraspinal muscles via the thoracolumbar fascia, thereby permitting load transfer from the lumbopelvic area to the lower extremities.
Therefore, as the insertions of the gluteus maximus into the ITT and thoracolumbar fascia, this muscle becomes important for the mechanical coordination of the lumbar, pelvic and lower limb areas. The fascial insertions of the gluteus maximus muscle could explain the transmission of forces from the thoracolumbar fascia to the knee, and consequently some types of referred pain to the lateral region of the thigh and leg.
Response from Clinical Anatomist John Sharkey to article on frozen shoulder following anaesthaesia.
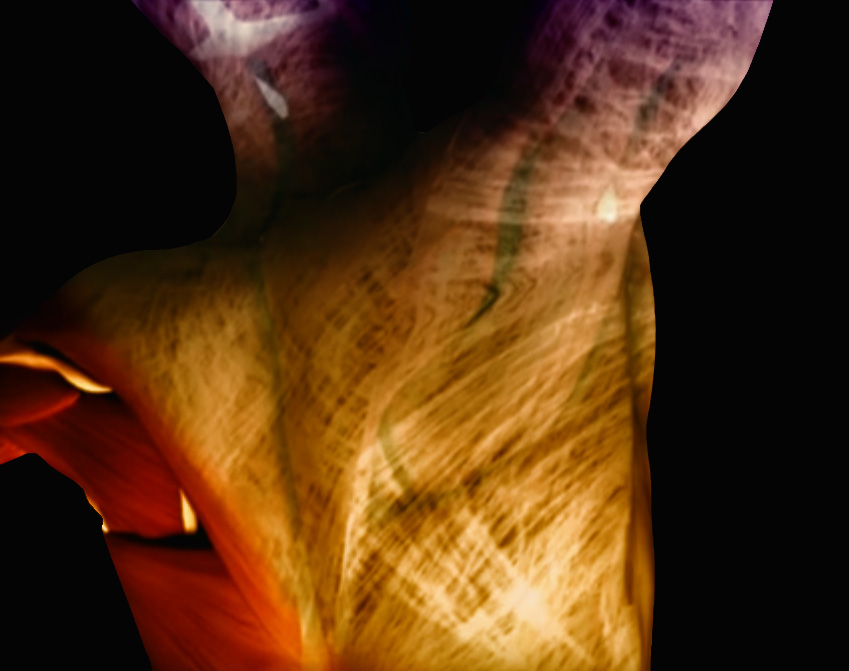
An interview with Dr. Jean-Claude Guimberteau